![]()
CPC練習AAPC高合格率回答あなたを試験は高確率で合格させます![2025]
最高の方法からパスCertified Professional CoderのCPC試験合格させます
質問 # 58
This 27-year-old male has morbid obesity with a BMI of 45 due to a high calorie diet. He has decided to have an open Roux-en-Y gastric bypass. The patient is brought to the operating room and placed in supine position. A midline abdominal incision is made. The stomach is mobilized, and the proximal stomach is divided and stapled creating a small proximal pouch in continuity with the esophagus. A short limb of the proximal bowel of 155 cm is divided. It is brought up and anastomosed to the gastric pouch. The other end of the divided bowel is connected back into the distal small bowel to the short limb's gastric anastomosis to restore intestinal continuity. The abdominal incision is closed.
What are the procedure and diagnosis codes for this encounter?
- A. 43847, E66.9, Z68.42
- B. 43645, E66.8, Z68.42
- C. 43644, E66.01, Z68.43
- D. 43847, E66.01, Z68.42
正解:D
質問 # 59
A surgeon performs midface LeFort I reconstruction on a patient's facial bones to correct a congenital deformity. The reconstruction is performed in two pieces in moving the upper jawbone forward and repositioning the teeth of the maxilla of the mid face.
What CPT code is reported?
- A. 0
- B. 1
- C. 2
- D. 3
正解:C
質問 # 60
A 45-year-old female presents to the ED with chest pain. The provider has an Albumin Cobalt Binding Test to determine if the chest pain is ischemic in nature.
That lab test is reported?
- A. 0
- B. 1
- C. 2
- D. 3
正解:D
解説:
* Procedure: Albumin Cobalt Binding (ACB) test to determine ischemic nature of chest pain.
* CPT Code:
* 83857: This code is used for the Albumin Cobalt Binding test.
* Code Selection Justification: The ACB test specifically measures ischemia-modified albumin, making
83857 the appropriate code for this laboratory test.
References:
* AMA CPT Professional Edition (current year)
* ICD-10-CM (current year)
* HCPCS Level II (current year)
質問 # 61 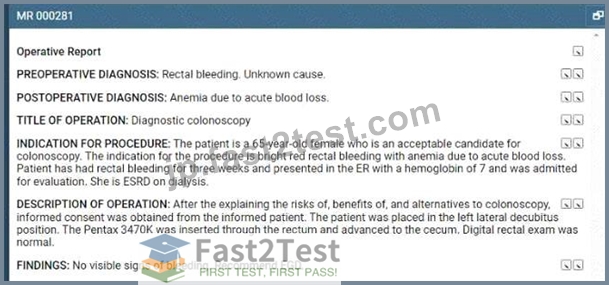
Refer to the supplemental information when answering this question:
View MR 000281
What anesthesia and diagnosis codes are reported for this case?
- A. 00812, D62, N18.6, Z99.2
- B. 00811, D64.9, K62.5, N18.6, Z99.2
- C. 00812, D64.9, K62.5, N18.6, Z99.2
- D. 00811, D62, N18.6, Z99.2
正解:D
解説:
* CPT Code 00811: Anesthesia for lower intestinal endoscopic procedures, endoscope introduced distal to the splenic flexure; diagnostic, with or without collection of specimen(s) by brushing or washing
* This code is reported for anesthesia services provided during a colonoscopy that is diagnostic in nature.
* ICD-10-CM Code D62: Acute posthemorrhagic anemia
* This is the most accurate postoperative diagnosis. The operative report states "Anemia due to acute blood loss."
* ICD-10-CM Code N18.6: End stage renal disease
* This code captures the patient's documented history of ESRD.
* ICD-10-CM Code Z99.2: Dependence on renal dialysis
* This code is necessary to report the patient's dialysis status, as it affects the overall risk of the procedure.
Why other options are incorrect:
* 00812: This code is for therapeutic colonoscopies, not diagnostic.
* D64.9: This code is for anemia, unspecified. D62 is more specific to the patient's condition.
* K62.5: This code is for lower gastrointestinal bleeding, but the anemia is the primary diagnosis in this case.
References:
* CPT Code 00811: Anesthesia for lower intestinal endoscopic procedures, endoscope introduced distal to the splenic flexure; diagnostic, with or without collection of specimen(s) by brushing or washing
* ICD-10-CM Code D62: Acute posthemorrhagic anemia
* ICD-10-CM Code N18.6: End stage renal disease
* ICD-10-CM Code Z99.2: Dependence on renal dialysis
* AAPC Coder's Desk Reference: This resource provides detailed information on coding guidelines and procedures.
質問 # 62
A 1-year-old is with his mom to have his scheduled vaccinations. The physician provides counseling for routine immunizations and carries out measles, mumps, rubella and varicella (MMRV) subcutaneously and dose 3 of Hepatitis B intramuscularly without difficulty.
What CPTcodes are reported?
- A. 90460, 90461, 90710, 90744
- B. 90471, 90472, 90707, 90746
- C. 90460 x 2, 90461 x 3, 90710, 90744
- D. 90471, 90472 x 4, 90707, 90746
正解:C
解説:
1. Procedure and CPTCode Selection:
The physician administered the MMRV (measles, mumps, rubella, and varicella) vaccine subcutaneously and dose 3 of Hepatitis B vaccine intramuscularly. The physician also provided counseling on routine immunizations.
CPTCode 90460 is used for immunization administration with counseling by the physician for patients 18 years or younger for the first or only component of each vaccine.
CPTCode 90461 is used for each additional component in a vaccine with counseling.
90710 is the code for the MMRV vaccine.
90744 is the code for the Hepatitis B vaccine (pediatric).
2. Application of 90460 and 90461:
For the MMRV vaccine (which has four components: measles, mumps, rubella, and varicella), 90460 is reported once for the first component, and 90461 is reported three times (once for each additional component).
For the Hepatitis B vaccine, 90460 is reported again since it is a separate vaccine with one component.
3. Rationale for Excluding Other Options:
Option A (90471, 90472 x 4, 90707, 90746) uses codes for vaccine administration without counseling and incorrect vaccine codes (90707 for MMR instead of MMRV and 90746 for adult Hepatitis B instead of pediatric).
Option B and Option D also contain incorrect vaccine codes and do not correctly apply the counseling administration codes.
4. AAPC and CPTCoding Guidelines:
According to AAPC guidelines, 90460 and 90461 are the appropriate administration codes for vaccines with counseling provided to pediatric patients, with each component of a multi-component vaccine coded separately.
Therefore, the correct answer is C. 90460 x 2, 90461 x 3, 90710, 90744.
質問 # 63
View MR 005398
MR 005398
Operative Report
Preoperative Diagnosis: Nonfunctioning right kidney with ureteral stricture.
Postoperative Diagnosis: Nonfunctioning right kidney with ureteral stricture.
Procedure: Right nephrectomy with partial ureterectomy.
Findings and Procedure: Under satisfactory general anesthesia, the patient was placed in the right flank position. Right flank and abdomen were prepared and draped out of the sterile field. Skin incision was made between the 11th and 12th ribs laterally. The incision was carried down through the underlying subcutaneous tissues, muscles, and fascia. The right retroperitoneal space was entered. Using blunt and sharp dissection, the right kidney was freed circumferentially. The right artery, vein, and ureter were identified. The ureter was dissected downward where it is completely obstructed in its distal extent. The ureter was clipped and divided distally. The right renal artery was then isolated and divided between 0 silk suture ligatures. The right renal vein was also ligated with suture ligatures and 0 silk ties. The right kidney and ureter were then submitted for pathologic evaluation. The operative field was inspected, and there was no residual bleeding noted, and then it was carefully irrigated with sterile water. Wound closure was then undertaken using 0 Vicryl for the fascial layers, 0 Vicryl for the muscular layers, 2-0 chromic for subcutaneous tissue, and clips for the skin. A Penrose drain was brought out through the dependent aspect of the incision. The patient lost minimal blood and tolerated the procedure well.
What CPT coding is reported for this case?
- A. 0
- B. 1
- C. 2
- D. 3
正解:D
解説:
The procedure involves a right nephrectomy with partial ureterectomy for a nonfunctioning right kidney with ureteral stricture.
* Procedure Description:
* Right nephrectomy (removal of the kidney).
* Partial ureterectomy (removal of part of the ureter).
* CPT Coding:
* 50220: Nephrectomy, including partial ureterectomy, any open approach.
References:
* AMA's CPT Professional Edition (current year).
* CPT Assistant for detailed coding guidelines on nephrectomy procedures.
質問 # 64
A patient with malignant lymphoma is administered the antineoplastic drug Rituximab 800 mg and then 100 mg of Benadryl.
Which HCPCS Level II codes are reported for both drugs administered intravenously?
- A. J9312, Q0163
- B. J9312, J1200
- C. J9312 x 80, 00163 x 2
- D. J9312 x 80, J1200 x 2
正解:B
解説:
The patient with malignant lymphoma is administered Rituximab (800 mg) and Benadryl (100 mg) intravenously.
* Procedure Description:
* Administration of Rituximab (800 mg) intravenously.
* Administration of Benadryl (100 mg) intravenously.
* HCPCS Level II Coding:
* J9312: Injection, Rituximab, 10 mg.
* For 800 mg, report 80 units of J9312.
* J1200: Injection, Diphenhydramine HCl, up to 50 mg.
* For 100 mg, report 2 units of J1200.
References:
* HCPCS Level II Code Book (current year).
* HCPCS Level II coding guidelines for intravenous drug administration.
質問 # 65
Patient has cervical spondylosis with myelopathy. The surgeon performed a bilateral posterior laminectomy with facetectomies at each level and foraminotomies performed between interspaces C5-C6 and C6-C7. Bilateral decompression of the nerve roots is achieved.
What CPT coding is reported?
- A. 63045, 63048
- B. 0
- C. 63050-50
- D. 63040-50, 63043, 63043
正解:A
質問 # 66
Mr. Woolridge has had a suspicious lesion on his left shoulder for approximately eight weeks that is not healing. On the dermatologist's exam of left shoulder blade, there is excoriation and scabbing and the lesion not healing. Patient agrees and wishes to proceed with a punch biopsy of the lesion. A punch biopsy is taken of the lesion and sent to pathology. A simple repair is performed at the biopsy site.
What CPT and ICD-10-CM codes are reported?
- A. 11102, L98.9
- B. 11102, 12001-51, D49.2
- C. 11104,12001-51, L98.9
- D. 11104, D49.2
正解:B
解説:
CPT code 11102 is for punch biopsy of skin, including simple closure. CPT code 12001-51 is for simple repair of superficial wounds, with modifier 51 indicating multiple procedures. ICD-10-CM code D49.2 is used for a neoplasm of unspecified behavior of the bone, soft tissue, and skin. This coding accurately reflects the punch biopsy and simple repair performed on the lesion.References: AMA's CPT Professional Edition (current year), ICD-10-CM (current year)
質問 # 67
View MR 007400
MR 007400
Radiology Report
Patient: J. Lowe Date of Service: 06/10/XX
Age: 45
MR#: 4589799
Account #: 3216770
Location: ABC Imaging Center
Study: Mammogram bilateral screening, all views, producing direct digital image Reason: Screen Bilateral digital mammography with computer-aided detection (CAD) No previous mammograms are available for comparison.
Clinical history: The patient has a positive family history (mother and sister) of breast cancer.
Mammogram was read with the assistance of GE iCAD (computerized diagnostic) system.
Findings: No dominant speculated mass or suspicious area of clustered pleomorphic microcalcifications is apparent Skin and nipples are seen to be normal. The axilla are unremarkable.
What CPT coding is reported for this case?
- A. 77066, Z80.3, Z12.31
- B. 77066-50, Z12.31, Z80.3
- C. 77067, Z12.31, Z80.3
- D. 77067-50, Z80.3, Z12.31
正解:C
質問 # 68
View MR 005398
MR 005398
Operative Report
Preoperative Diagnosis: Nonfunctioning right kidney with ureteral stricture.
Postoperative Diagnosis: Nonfunctioning right kidney with ureteral stricture.
Procedure: Right nephrectomy with partial ureterectomy.
Findings and Procedure: Under satisfactory general anesthesia, the patient was placed in the right flank position. Right flank and abdomen were prepared and draped out of the sterile field. Skin incision was made between the 11th and 12th ribs laterally. The incision was carried down through the underlying subcutaneous tissues, muscles, and fascia. The right retroperitoneal space was entered. Using blunt and sharp dissection, the right kidney was freed circumferentially. The right artery, vein, and ureter were identified. The ureter was dissected downward where it is completely obstructed in its distal extent. The ureter was clipped and divided distally. The right renal artery was then isolated and divided between 0 silk suture ligatures. The right renal vein was also ligated with suture ligatures and 0 silk ties. The right kidney and ureter were then submitted for pathologic evaluation. The operative field was inspected, and there was no residual bleeding noted, and then it was carefully irrigated with sterile water. Wound closure was then undertaken using 0 Vicryl for the fascial layers, 0 Vicryl for the muscular layers, 2-0 chromic for subcutaneous tissue, and clips for the skin. A Penrose drain was brought out through the dependent aspect of the incision. The patient lost minimal blood and tolerated the procedure well.
What CPT coding is reported for this case?
- A. 0
- B. 1
- C. 2
- D. 3
正解:D
質問 # 69
Patient is diagnosed with dacryocystitis, which is the inflammation of?
- A. Fingernail
- B. Eardrum
- C. Cornea
- D. Lacrimal sac
正解:D
解説:
Dacryocystitis is the inflammation of the lacrimal sac, which is part of the tear drainage system located in the inner corner of the eye. The lacrimal sac is connected to the nasolacrimal duct, which drains tears into the nasal cavity. Inflammation in this area can cause pain, redness, and swelling near the inner corner of the eye.
References: ICD-10-CM, medical dictionaries
質問 # 70
A 60-year-old male has three-vessel disease and supraventricular tachycardia which has been refractory to other management. He previously had pacemaker placement and stenting of LAD coronary artery stenosis, which has failed to solve the problem. He will undergo CABG with autologous saphenous vein and an extensive modified MAZE procedure to treat the tachycardia.
He is brought to the cardiac OR and placed in the supine position on the OR table. He is prepped and draped, and adequate endotracheal anesthesia is assured. A median sternotomy incision is made and cardiopulmonary bypass is initiated. The endoscope is used to harvest an adequate length of saphenous vein from his left leg. This is uneventful and bleeding is easily controlled. The vein graft is prepared and cut to the appropriate lengths for anastomosis. Two bypasses are performed: one to the circumflex and another to the obtuse marginal. The left internal mammary is then freed up and it is anastomosed to the ramus, the first diagonal, and the LAD. An extensive maze procedure is then performed and the patient is weaned from bypass. At this point, the sternum is closed with wires and the skin is reapproximated with staples. The patient tolerated the procedure without difficulty and was taken to the PACU.
Choose the procedure codes for this surgery.
- A. 33535, 33259, 33519, 33508
- B. 33533, 33257-51, 33519-51, 33508-51
- C. 33535, 33259 51, 33519-51, 33508-51
- D. 33533, 33257, 33519, 33508
正解:D
質問 # 71
View MR 003396
MR 003396
Operative Report
Preoperative Diagnosis: Acute MI, severe left main arteriosclerotic coronary artery disease Postoperative Diagnosis: Acute MI, severe left main arteriosclerotic coronary artery disease Procedure Performed: Placement of an intra-aortic balloon pump (IABP) right common femoral artery Description of Procedure: Patient's right groin was prepped and draped in the usual sterile fashion. Right common femoral artery is found, and an incision is made over the artery exposing it. The artery is opened transversely, and the tip of the balloon catheter was placed in the right common femoral artery. The balloon pump had good waveform. The balloon pump catheter is secured to his skin after local anesthesia of 2 cc of 1% Xylocaine is used to numb the area. The balloon pump is secured with a 0-silk suture. The patient has sterile dressing placed. The patient tolerated the procedure. There were no complications.
What CPT coding is reported for this case?
- A. 0
- B. 1
- C. 2
- D. 3
正解:B
質問 # 72
A 5-year-old is brought to the QuickCare in the ED to repair two lacerations: a 3 cm laceration on her right arm and 2 cm laceration on her nose. Her arm is repaired with a simple one-layer closure with sutures. Her nose is repaired with a simple repair using tissue adhesive, 2-cyanoacrylate.
How are the repairs reported?
- A. 12002, 12011-59
- B. 0
- C. 1
- D. 12032, 12041-59
正解:C
質問 # 73
A mother brings her 2-year-old son to the pediatrician's office because he stuck a bead up his left nostril. The pediatrician uses a nasal decongestant to open the blocked nostril and removes the bead with nasal forceps.
What CPT coding is reported?
- A. 0
- B. 30300-50
- C. 30210-50
- D. 1
正解:A
質問 # 74
An elderly patient comes into the emergency department (ED) with shortness of breath. An ECG is performed The final diagnosis at discharge is impending myocardial infarction.
According to ICD-10-CM guidelines, how is this reported?
- A. I21.3, R06.02
- B. I20.0, R06.02
- C. I20.0
- D. R06.02
正解:D
質問 # 75
View MR 099405
MR 099405
CC: Shortness of breath
HPI: 16-year-old female comes into the ED for shortness of breath for the last two days. She is an asthmatic.
Current medications being used to treat symptoms is Advair, which is not working and breathing is getting worse. Does not feel that Advair has been helping. Patient tried Albuterol for persistent coughing, is not helping. Coughing 10-15 minutes at a time. Patient has used the Albuterol 3x in the last 16 hrs. ED physician admits her to observation status.
ROS: No fever, no headache. No purulent discharge from the eyes. No earache. No nasal discharge or sore throat. No swollen glands in the neck. No palpitations. Dyspnea and cough. Some chest pain. No nausea or vomiting. No abdominal pain, diarrhea, or constipation.
PMH: Asthma
SH: Lives with both parents.
FH: Family hx of asthma, paternal side
ALLERGIES: PCN-200 CAPS. Allergies have been reviewed with child's family and no changes reported.
PE: General appearance: normal, alert. Talks in sentences. Pink lips and cheeks. Oriented. Well developed.
Well nourished. Well hydrated.
Eyes: normal. External eye: no hyperemia of the conjunctiva. No discharge from the conjunctiva Ears: general/bilateral. TM: normal. Nose: rhinorrhea. Pharynx/Oropharynx: normal. Neck: normal.
Lymph nodes: normal.
Lungs: before Albuterol neb, mode air entry b/l. No rales, rhonchi or wheezes. After Albuterol neb.
improvement of air entry b/l. Respiratory movements were normal. No intercostals inspiratory retraction was observed.
Cardiovascular system: normal. Heart rate and rhythm normal. Heart sounds normal. No murmurs were heard.
GI: abdomen normal with no tenderness or masses. Normal bowel sounds. No hepatosplenomegaly Skin: normal warm and dry. Pink well perfused Musculoskeletal system patient indicates lower to mid back pain when she lies down on her back and when she rolls over. No CVA tenderness.
Assessment: Asthma, acute exacerbation
Plan: Will keep her in observation overnight. Will administer oral steroids and breathing treatment. CXR ordered and to be taken in the morning.
What E/M code is reported?
- A. 0
- B. 1
- C. 2
- D. 3
正解:B
解説:
* 99222: This code is used for initial hospital care, per day, for the evaluation and management of a patient, which requires a detailed or comprehensive history, a detailed or comprehensive examination, and medical decision making of moderate complexity.
* The documentation shows a detailed history (including HPI, ROS, PMH, SH, and FH) and a detailed examination (covering multiple organ systems). The medical decision making involves the management of an acute asthma exacerbation, which includes admitting the patient to observation status, administering oral steroids, and planning for further diagnostic testing.
References:
* CPT Professional Edition, AMA
質問 # 76
View MR 099401
MR 099401
Established Patient Office Visit
Chief Complaint: Patient presents with bilateral thyroid nodules.
History of present illness: A 54-year-old patient is here for evaluation of bilateral thyroid nodules. Thyroid ultrasound was done last week which showed multiple thyroid masses likely due to multinodular goiter.
Patient stated that she can "feel" the nodules on the left side of her thyroid. Patient denies difficulty swallowing and she denies unexplained weight loss or gain. Patient does have a family history of thyroid cancer in her maternal grandmother. She gives no other problems at this time other than a palpable right-sided thyroid mass.
Review of Systems:
Constitutional: Negative for chills, fever, and unexpected weight change.
HENT: Negative for hearing loss, trouble swallowing and voice change.
Gastrointestinal: Negative for abdominal distention, abdominal pain, anal bleeding, blood in stool, constipation, diarrhea, nausea, rectal pain, and vomiting Endocrine: Negative for cold Intolerance and heat intolerance.
Physical Exam:
Vitals: BP: 140/72, Pulse: 96, Resp: 16, Temp: 97.6 °F (36.4 °C), Temporal SpO2: 97% Weight: 89.8 kg (198 lbs ), Height: 165.1 cm (65") General Appearance: Alert, cooperative, in no acute distress Head: Normocephalic, without obvious abnormality, atraumatic Throat: No oral lesions, no thrush, oral mucosa moist Neck: No adenopathy, supple, trachea midline, thyromegaly is present, no carotid bruit, no JVD Lungs: Clear to auscultation, respirations regular, even, and unlabored Heart: Regular rhythm and normal rate, normal S1 and S2, no murmur, no gallop, no rub, no click Lymph nodes: No palpable adenopathy ASSESSMENT/PLAN:
1) Multinodular goiter - the patient will have a percutaneous biopsy performed (minor procedure).
What E/M code is reported for this encounter?
- A. 0
- B. 1
- C. 2
- D. 3
正解:C
解説:
The patient is an established patient presenting with bilateral thyroid nodules and has a detailed history and examination performed.
* Procedure Description:
* Detailed history and examination of bilateral thyroid nodules.
* Review of systems and physical examination.
* Assessment and plan for a percutaneous biopsy.
* CPT Coding:
* 99214: Office or other outpatient visit for the evaluation and management of an established patient, which requires a medically appropriate history and/or examination and moderate medical decision making.
References:
* AMA's CPT Professional Edition (current year).
* CPT Assistant for detailed coding guidelines on evaluation and management services.
質問 # 77
An established patient suffering from migraines without aura, no mention of intractable migraine, and no mention of status migrainosus, is seen by his ophthalmologist who conducts a visual field examination of both eyes. The examination was accomplished plotting four isopters utilizing the Goldmann perimeter testing method. The patient and requesting physician receive the interpretation and report on the same date of service.
What procedure and diagnosis codes are reported for this encounter?
- A. 92082, G43.009
- B. 92082, G43.019
- C. 92081, G43.009
- D. 92083, G43.019
正解:A
解説:
* Procedure: Visual field examination of both eyes using Goldmann perimeter testing with four isopters.
* CPT Code:
* 92082: This code is for visual field examination with intermediate examination.
* ICD-10-CM Code:
* G43.009: Migraine without aura, not intractable, without status migrainosus.
* Code Selection Justification: The visual field exam method and complexity align with 92082. The patient's diagnosis of non-intractable migraine without aura is coded as G43.009.
References:
* AMA CPT Professional Edition (current year)
* ICD-10-CM (current year)
質問 # 78
The gastroenterologist performs a simple excision of three external hemorrhoids and one internal hemorrhoid, each lying along the left lateral column. The operative report indicates that the internal hemorrhoid is not prolapsed and is outside of the anal canal.
What CPT and ICD-10CM codes are reported?
- A. 46250, 46945, K64.0, K64.4
- B. 46255, K64.0, K64.4
- C. 46320, 46945, K64.0, K64.9
- D. 46250, K64.0, K64.9
正解:D
質問 # 79
A complete cardiac MRI for morphology and function without contrast, followed by contrast with four additional sequences and stress imaging, is performed on a patient with systolic left ventricular congestive heart failure and premature ventricular contractions.
What CPT and ICD-10-CM codes are reported?
- A. 75557, 75559, I50.1, I49.1
- B. 75561, 75563, I50.1, I49.1
- C. 75559, I50.20, I49.3
- D. 75563, I50.20, I49.3
正解:D
質問 # 80
A cardiologist attempted to perform a percutaneous transluminal coronary angioplasty of a totally occluded blood vessel. The surgeon stopped the procedure because of an anatomical problem creating risk for the patient and preventing performance of the catheterization.
What modifier is appended to the procedure code?
- A. 0
- B. 1
- C. 2
- D. 3
正解:C
解説:
Modifier 53 is used to report a discontinued procedure. It indicates that a procedure was started but terminated due to the patient's well-being being at risk. In this scenario, the percutaneous transluminal coronary angioplasty was attempted but stopped because of an anatomical problem that created a risk for the patient, preventing the completion of the procedure.References: AMA's CPT Professional Edition, coding guidelines on the use of modifiers.
質問 # 81 

Refer to the supplemental information when answering this question:
View MR 138093
What E/M coding is reported?
- A. 0
- B. 99291-25, 92950, 31500, 82803
- C. 99291-25, 99292-25, 92950, 31500
- D. 99285-25, 99291-25, 92950, 31500, 82803
正解:B
解説:
This patient presents to the ER with syncope, requiring a comprehensive evaluation and critical care. Here's the breakdown of the codes:
* CPT Code 99291-25: Critical care, evaluation and management of the critically ill or critically injured patient; first 30-74 minutes
* This code is appropriate because the patient's syncope and vital signs (low blood pressure, shallow respirations, low oxygen saturation) indicate a critical condition requiring immediate intervention.
* Modifier -25: Significant, Separately Identifiable Evaluation and Management Service by the Same Physician on the Same Day of the Procedure or Other Service. This modifier is appended because the critical care services were provided in addition to the separately reported procedures below.
* CPT Code 92950: Cardiopulmonary resuscitation (eg, CPR, external cardiac massage, endotracheal intubation, ventilation)
* While the documentation doesn't explicitly mention CPR, it states the patient was unresponsive upon arrival but had spontaneous pulse and respirations. This suggests possible resuscitation efforts were performed by the paramedics before the physician's assessment.
* CPT Code 31500: Intubation, endotracheal, emergency procedure
* Although not explicitly stated, the documentation indicates the patient was placed on "high flow oxygen," which strongly suggests endotracheal intubation was performed to manage the patient's respiratory distress.
* CPT Code 82803: Blood gases, arterial, pH, PCO2, PO2, with oxygen saturation; interpretation and report
* This code is likely reported based on the patient's respiratory distress and the need to monitor their oxygenation status.
Why other options are incorrect:
* 99285: This is a standard emergency department visit code and doesn't capture the critical nature of the patient's condition.
* 99285-25, 99291-25, 92950, 31500, 82803: This includes 99285, which is not necessary as 99291 encompasses the evaluation and management.
* 99291-25, 99292-25, 92950, 31500: This includes 99292, which is for subsequent critical care time.
There's no indication in the documentation that the physician provided critical care beyond the initial 74 minutes.
References:
* CPT Codes 99281-99285: Emergency department visits
* CPT Codes 99291-99292: Critical care services
* CPT Code 92950: Cardiopulmonary resuscitation
* CPT Code 31500: Endotracheal intubation
* CPT Code 82803: Arterial blood gases
* AAPC Coder's Desk Reference: This resource provides detailed information on coding guidelines and procedures.
質問 # 82
A patient is diagnosed with compression fractures of the C6, C7 and T1 vertebrae. The patient agrees to have vertebroplasty. Bone cement is injected in the vertebral space until each of the two whole vertebral body is filled. The procedure is performed bilaterally.
What CPTcoding is reported?
- A. 22513, 22515
- B. 22510, 22512 x 2
- C. 22510-50, 22512-50 x 2
- D. 22513-50, 22513-50
正解:C
解説:
1. Procedure Type and CPTCode Selection:
The physician performed an injection into the wrist joint for degenerative osteoarthritis management using Synvisc (a viscosupplementation product).
Code 20606 is the correct CPTcode for an arthrocentesis, aspiration, and/or injection procedure in an intermediate joint, such as the wrist. This code specifically includes the use of ultrasound guidance, which is often standard in such injections.
Code 20551 (injection of a single tendon origin) and 20526 (injection into a carpal tunnel) are incorrect here as they do not apply to intra-articular injections for joint osteoarthritis management.
2. Diagnosis Code Selection (ICD-10-CM):
The diagnosis is degenerative osteoarthritis in the right wrist.
ICD-10-CM Code M19.231 is used for primary osteoarthritis of the right wrist. This code directly reflects the diagnosis of primary osteoarthritis affecting this specific joint.
M19.031 would represent primary osteoarthritis in the wrist but does not specify laterality; therefore, it is less accurate than M19.231, which denotes the right wrist.
3. Summary of Code Application:
The correct CPTand ICD-10-CM codes are 20606 for the injection procedure and M19.231 for primary osteoarthritis of the right wrist.
4. AAPC and CPTCoding Guidelines:
According to AAPC CPC guidelines, proper joint injection codes require specific identification of the joint location and guidance if used. Additionally, selecting the most specific ICD-10-CM code for laterality is essential for accuracy in musculoskeletal diagnoses.
Thus, based on CPTand ICD-10-CM coding guidelines, the verified answer is B. 20606, M19.231.
質問 # 83
......
AAPC CPC 認定試験の出題範囲:
| トピック | 出題範囲 |
|---|---|
| トピック 1 |
|
| トピック 2 |
|
| トピック 3 |
|
| トピック 4 |
|
AAPC CPC事前に試験練習テストFast2test: :https://jp.fast2test.com/CPC-premium-file.html
CPC練習テスト問題回答解釈::https://drive.google.com/open?id=1E4xEWI38bJFCUicwvp7k_-WopHWXXOsf